Simplify Communications Between Your Practice and Ours
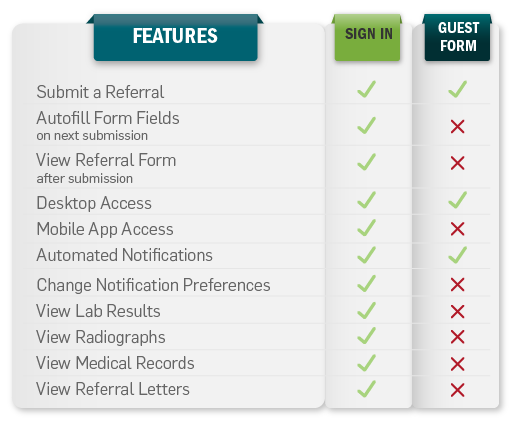
Submit patient referrals online and stay informed with automated notifications. Receive referral letters, and diagnostic and radiograph results electronically or by fax.
Sign in to the Portal Guest Referral Form Outpatient Ultrasound Referral
Portal Support
All members of your veterinary team will have online access to patient records through a shared username and password.
Contact us if you have questions, or if you need your password reset.
Self Help Video Tutorials and helpful starter guides.
Sign in to the Veterinary Portal
You can also sign in on a nice fresh window if you prefer. Click here for that.